By ANISH KOKA
I was listening to a conversation between two critical thinkers I respect greatly: geneticist/technologist/blogger Razib Khan and Washington Post columnist Megan McArdle. Their discussion was a freewheeling rant about the problems they see with the rise of populism on the left and right, but a throwaway comment related to the US physician shortage in the context of needing high skilled immigrant labor towards the end of the almost two-hour conversation made me realize how little people really know about healthcare in America. Of course, everyone knows certain aspects of healthcare as a consumer very well, but even if you are a high-IQ individual who can make use of the vast information at all of our fingertips, it is hard to really know what the reality on the ground is without living it / having deep knowledge. Interestingly enough, early on Megan and Razib both acknowledge the impossibility of commenting on the situation in Iran, because the Iraq war taught them the folly of making conclusions from the available information. Bottom line, it doesn’t matter how smart you are if your conclusions are based on reading Colin Powell on the weapons of mass destruction Saddam Hussein must have. The public may not realize it, but health policy has a similar problem. The vast majority of academics “covering” American health policy, and in charge of describing healthcare, are ideologues whose main goal is not to describe reality, but to fashion a story. And as any screenwriter will tell you — do not let the facts get in the way of a good story.
What follows is an examination of what happens when you pull one of the important healthcare threads that forms the bedrock of many healthcare opinions that smart people like Megan and Razib hold: Rural access to healthcare in America.
First, here’s what a Google search reveals — and notice the sources. I assure you that PubMed is not much different. Rural healthcare access in America must be bad, right?
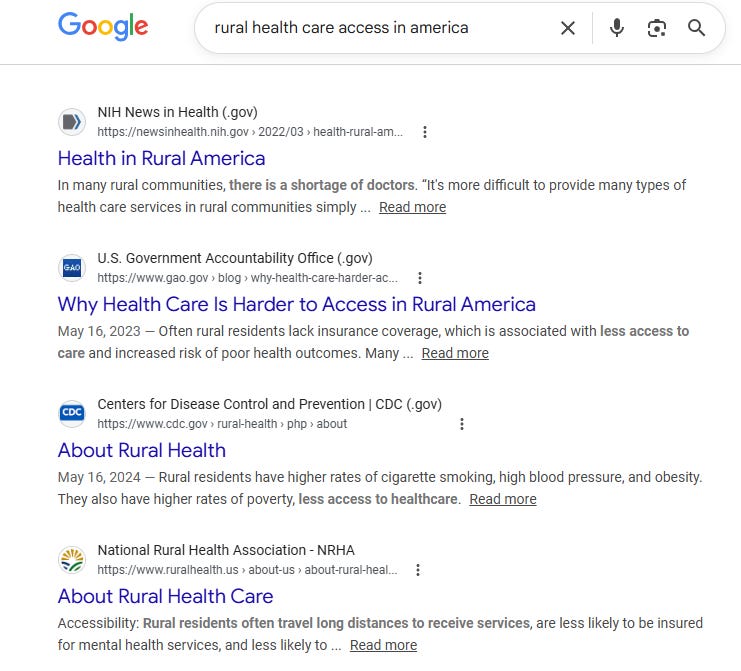
Once we establish that healthcare access in rural America is “bad”, there are all sorts of conclusions that are downstream from that like funding of rural hospitals, and management of the physician labor supply.
But the strange thing about the rural healthcare access problem that should strike anyone over a certain age that has followed/lived healthcare is that we have been talking about this and passing legislation on the matter forever, and yet if you are to believe those who should have the most knowledge about these things, we continue to fall short.
Understanding what exactly is happening requires some knowledge of the legislative sausage that has created the current landscape. Understanding the laws and more importantly how they are implemented should quickly make the reader understand why there is a powerful incentive to maintain a certain narrative.
A brief summary of some major legislation currently on the books exposes exactly why it may be so important to maintain a certain narrative on rural health care access.
The Critical Access Hospital (CAH) designation, created by the Balanced Budget Act of 1997 after a wave of rural closures, gave over 1,300 hospitals cost-based Medicare reimbursement — meaning Medicare pays whatever the hospital reports it cost to deliver the service.
The Rural Health Care Access Act of 2025 (H.R. 771) goes further, eliminating the distance requirement that a hospital must be more than 35 miles from another hospital to qualify as a CAH, extending cost-based reimbursement to hospitals that were never remote enough to meet the original threshold.
The Rural Emergency Hospital (REH) designation allows low-volume rural hospitals to drop inpatient beds while retaining emergency and outpatient services — and receiving additional federal payments — with recent legislation proposing to extend eligibility to hospitals that closed as far back as 2014.
Congress has also allocated new Medicare-funded Graduate Medical Education (GME) residency slots specifically for rural hospitals, even though a December 2025 GAO report found that 95 percent of the hospitals receiving slots were geographically urban hospitals that had legally reclassified themselves as rural to qualify.
The Rural Health Focus Act formally authorizes the CDC Office of Rural Health with dedicated appropriations, and the Fair Funding for Rural Hospitals Act modernizes disproportionate share hospital payments with a $20 million per-state funding floor.
Perhaps most consequentially, one of the primary political shields against site-neutral payment reform — the policy that would equalize Medicare reimbursement regardless of whether a service is delivered in a hospital outpatient department or a physician’s office — a change that would save Medicare tens of billions annually comes from those arguing that this change would close hundreds of rural hospitals within six months.
Every one of these programs represents a funding line. And every attempt to close the loopholes in these programs is quickly crushed with an avalanche of moralizing about saving money on the back of the indigent. You can understand that there are a lot of interests that have much to gain by promulgating a rural health care access gap. Nowhere is the spin on American healthcare more obvious than when it falls to academics to critique it. Academic health policy wonks nationally and internationally consistently rank American healthcare as woefully inadequate relative to our peer nations that have some form of nationalized/socialized healthcare.
This narrative has a powerful institutional home. The Commonwealth Fund’s Mirror Mirror report, probably the most widely cited international healthcare comparison, has ranked the United States last or near-last among high-income countries in virtually every edition for the past two decades. The report’s methodology leans heavily on insurance coverage, administrative burden, equity metrics, and survey-based measures of patient experience. Countries with national insurance systems — the United Kingdom, Canada, and the Nordic countries — score well on the access dimension almost by definition, because universal coverage is treated as equivalent to universal access. The American system, with its patchwork of private insurance, Medicaid, and Medicare performs poorly on these metrics and gets ranked accordingly. These rankings are then cited in congressional testimony, think-tank reports, and op-ed pages as evidence that the American healthcare system is inferior — that Americans get less for more, and that a national insurance program would fix it.
But what good is a national insurance card if there is no hospital within the critical 90 minute time window when you have a heart attack? Insurance coverage and geographic access to care are not the same thing. A patient in rural Canada has universal coverage but may wait hours for an ambulance to reach a cardiac cath lab — if one is reachable at all. A patient in rural Nevada may be uninsured and be at a PCI-capable hospital in 40 minutes. The former is counted as “access” in the Commonwealth Fund framework. The latter is counted as a failure. The rankings measure the bureaucratic architecture of insurance systems, not the physical reality of whether care can be delivered, especially when it is most urgently needed.
So how about we actually try to quantify the American patchwork and compare it to one of our peer nations that is supposed to be a model for us — our Medicare for All Canadian neighbor.
Percutaneous coronary intervention — the procedure that opens a blocked coronary artery during a heart attack — is close to an ideal proxy for healthcare access broadly. It is definitionally time-sensitive: the ACC/AHA guidelines set a 90-minute door-to-balloon target for a reason, and delays beyond that threshold carry measurable mortality/morbidity consequences. It requires significant infrastructure — a catheterization laboratory, trained interventional cardiologists, a specialized team available around the clock. It is therefore not uniformly distributed across geographies. And crucially, it is a procedure where we have excellent public data on exactly where it is being performed.
Access to PCI is not a perfect proxy for access to all medical care. But if a community has a functioning PCI program within reasonable distance, it almost certainly has the broader infrastructure — emergency services, hospital beds, advanced imaging, specialist coverage — that defines a functional healthcare ecosystem. The inverse is also roughly true: communities far from PCI tend to be far from the rest of advanced care as well. PCI access is a reasonable healthcare canary.
When you measure the actual distance between where Americans live and where the nearest cath lab is — using real hospital data and population-weighted geography — what do we find?
Building the maps — and what they show
How the U.S. map was built
The foundation is a 2006 paper by Nallamothu et al. in Circulation — still the most rigorous published analysis of geographic PCI access in the United States — which found that 84% of Americans live within 60 minutes of a PCI-capable hospital. Using Medicare billing records for DRG codes 246–251 to identify 1,322 hospitals actively performing PCI, and replicating the Nallamothu methodology with updated data, I find essentially the same result. No comparable developed nation approaches this level of access — and I will get to what the closest peer comparisons actually look like below.
But a simple county choropleth — color each county by drive time — has a fundamental problem: it treats a county of 600 people identically to one of 600,000. The vast empty counties of the interior West look alarming on the map, and their sheer geographic mass dominates the visual.
The policy-relevant question is not which counties are far from PCI, but whether the people who live in those counties are far from PCI — and whether the population density in those areas justifies the kind of infrastructure investment the rural access narrative calls for.
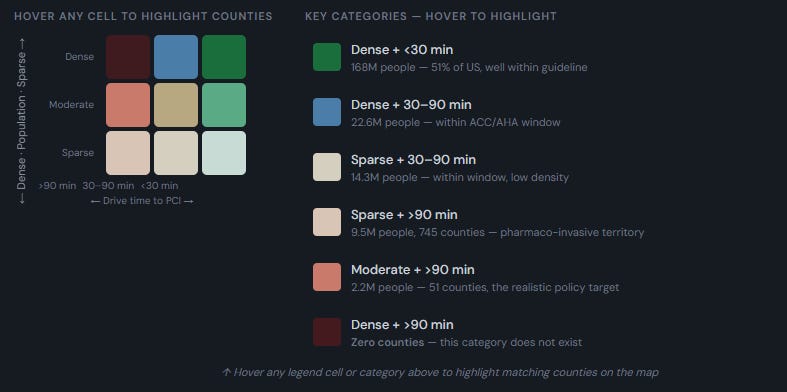
To answer the question I built a bivariate map encoding both dimensions, population density, and distance to a PCI-capable hospital. Counties are assigned to three density categories using the 50th and 90th percentiles of the county density distribution — percentile-based thresholds rather than arbitrary absolute cutoffs.

I then defined three access bands anchored to the ACC/AHA guideline for opening a blocked artery in the setting of an acute heart attack: within 30 minutes, 30 to 90 minutes, and beyond 90 minutes. Beyond 90 minutes is an important threshold that defines the point where most individuals will have a cardiac scar or worse if they are outside this time window for artery opening.
The centroid problem — and why it matters
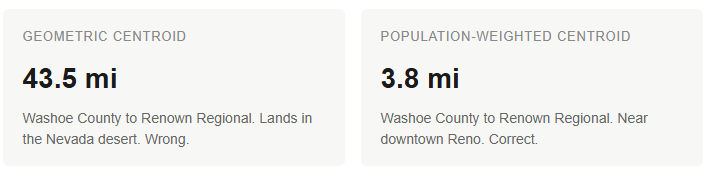
Creating a database of drive time from a hospital requires defining where to measure from. The United States is separated into counties, and taking the geographic center of the county (the geographic centroid) as the distance to measure from creates some meaningless distortions because the population in any given county is not necessarily clustered in the middle of the county. Large western counties where nearly all the population is clustered in one corner of a vast area explain why the simple geographic centroid fails so badly.

Click on the map to be taken to an interactive map
Reno sits in the southwest corner of Washoe County, home to Renown Regional Medical Center and St. Mary’s Regional. But Washoe County extends hundreds of miles into the Nevada desert. Its geometric centroid lands 43.5 miles from Renown, in an area where essentially nobody lives — and an earlier version of a map I made marked it red. Luckily, the Census Bureau publishes population-weighted centroids for all 3,143 U.S. counties in the CenPop2020 file, calculated from 2020 block-level data. Washoe’s population-weighted centroid is 3.8 miles from Renown. That is the correct number, and so I used population-weighted centroids for every U.S. county.
What the U.S. map actually shows
The striking finding is not about dense counties — dense counties cluster around cities, and cities have hospitals. The striking finding is about the moderate and sparse counties: even at low population densities, a surprisingly large share of the American population is within the 90-minute guideline window. But despite the enormous federal apparatus dedicated to rural healthcare access, 2.2 million Americans in moderate-density counties and 9.5 million in sparse counties — roughly 11.7 million total, or about 3.5% of the population — live beyond 90 minutes from a PCI hospital. Those are the people the rural access legislation is ostensibly built for, and after decades of CAH designations, GME slot carve-outs, Rural Emergency Hospital programs, and billions in cost-based reimbursement, that is what remains.

Click on the map for an interactive version
The peer comparison problem — the U.S. is genuinely without peers
Every international comparison of healthcare access implicitly assumes the countries being compared are meaningfully comparable. They are not — at least not for this question. The United States is the third-largest country in the world by land area and the third most populous. No high-income democracy comes close to combining both. The United Kingdom has 68 million people in an area smaller than Oregon. The Nordic countries together have fewer people than the greater New York metropolitan area spread across a landmass that is mostly accessible by road. These countries face no meaningful analog to the American geographic access problem.
The countries that do approximate the U.S. in scale — Russia, China, India, Brazil — fail so comprehensively on PCI access that no meaningful comparison is possible. Russia has perhaps 100 PCI centers for 144 million people across 11 time zones. China’s cath lab infrastructure is heavily concentrated in coastal cities. India and Brazil have dramatic urban-rural gradients at a severity that makes rural Nevada look well-served. These are not peer comparators. They are cautionary tales about what actually happens when healthcare infrastructure is insufficient at continental scale.
This is why international access rankings that place the United States alongside Belgium, the Netherlands, and New Zealand are not measuring the same thing. A country the size of Maryland with universal insurance and three PCI centers serving a compact population is not navigating the same access challenge as a country spanning four time zones with 335 million people. The Commonwealth Fund framework does not account for this, but the bivariate maps do.
Canada: the closest legitimate comparison — and a sobering one
Canada is the most defensible peer comparison — similar legal and institutional tradition, similar income level, physically adjacent, and frequently invoked by American reform advocates as a model. But making the Canadian map involved different choices than the U.S. map.
The Canadian map uses census divisions rather than counties — there are 282 of them, compared to 3,143 U.S. counties. PCI center locations were compiled from CIHI Cardiac Care Quality Indicators and provincial cardiac network directories rather than from a Medicare billing equivalent, because Canada has no public analog to the CMS procedure-level data. The 30 centers identified are the best available count, but the sourcing is less rigorous than the U.S. approach.
More importantly, the density thresholds for Canada are calculated separately from Canadian census division percentiles — sparse below 17 per square mile, moderate 17 to 213, dense above 213 — rather than applying U.S. thresholds. Canada is just so darn sparsely populated overall that applying U.S. density thresholds would classify virtually every Canadian census division as sparse, collapsing the bivariate analysis into a single meaningless category. Even with Canada-specific thresholds that are far more forgiving than U.S. ones (what counts as “dense” in Canada would be “moderate” in the United States) the comparison is still stark.

Baber et al. in Open Medicine (2011) found that 63.9% of Canadians aged 40 and older live within 60 minutes of a PCI facility, versus 84% of Americans. That 20-point gap reflects a country where 30 PCI centers serve 38 million people spread across the world’s second-largest landmass, concentrated almost entirely within 125 miles of the U.S. border. Applying the same bivariate methodology, approximately 10.9 million Canadians — 28.7% of the total population — live beyond 90 minutes from a PCI hospital. That includes:
- 4.4 million in sparse census divisions beyond 90 minutes (11.5% of population)
- 5.5 million in moderate-density census divisions beyond 90 minutes (14.4%)
- 1.1 million in dense census divisions beyond 90 minutes (2.8%) — a category that contains zero Americans
Those 1.1 million Canadians in dense-but-far census divisions represent the starkest contrast with the United States. They are concentrated in the Quebec City–Trois-Rivières corridor — a populated, accessible stretch of southern Quebec that in any reasonable sense should be well-served. And yet, remarkably, it isn’t.
I manually checked this to make sure the code was correct. Here are the four dense census divisions and their nearest PCI hospitals:
- Francheville (Trois-Rivières area, 452,604 people): nearest PCI is the Institut universitaire de cardiologie et de pneumologie de Québec — 54.6 miles, estimated 110 minutes
- D’Autray (Berthierville area, 266,948 people): nearest PCI is the Montreal Heart Institute — 53.4 miles, estimated 108 minutes
- Shawinigan (195,640 people): nearest PCI is the Institut universitaire de cardiologie — 75.9 miles, estimated 147 minutes
- Montmagny (east of Quebec City, 150,022 people): nearest PCI is the Institut universitaire de cardiologie — 47.9 miles, estimated 98 minutes
To put the overall numbers in context: the U.S., with nearly nine times Canada’s population, has 11.7 million people beyond the 90-minute threshold — 3.5% of its population. Canada has 10.9 million beyond the threshold out of 38 million — 28.7%. On a per-capita basis, Canada’s access gap is roughly eight times worse than America’s, in a country where 90% of the population lives in a narrow temperate corridor along the world’s longest undefended border. A simple framing of American rural access as a crisis that demands X while holding up Canadian Medicare as a model tells me you are either uninformed or have a dog in the fight.
So where does this leave us?
The United States is not perfect. Eleven point seven million Americans live beyond the 90-minute window for emergency cardiac care, and that matters. Every one of those people deserves better. But the honest framing of that number is that it represents 3.5% of the population of a continent-spanning nation — and that no comparable country on earth comes close to matching it. Canada, the country most frequently held up as the model America should follow, leaves 28.7% of its population outside that same window, including over a million people in densely populated (by Canada standards) areas. Rural healthcare access is a genuinely hard problem at continental scale and the headline should be that the United States has solved more of that problem than anyone else.
And yet this is not the story you will read in the Commonwealth Fund reports, or in the health policy journals, or in the congressional testimony that precedes the next round of rural hospital funding. The dominant narrative — that American rural healthcare is in crisis, that we are falling behind our peers, that the system is failing — is maintained by two groups with aligned incentives. The first is the academic and advocacy class that wants a government-payer system and needs American healthcare to look broken to justify the overhaul. The Canadian comparison is instructive: the single-payer system they want Americans to adopt delivers measurably worse geographic access to emergency cardiac care than the patchwork they want to replace. The second group is the healthcare industry itself — the health systems, the hospital associations, the administrators of residency training programs and the hospitals that are all too happy to take advantage of a Medicare funded program that gives them free physician labor. All of this is fueled by funding streams that, in part, depend on the continued perception of a rural access crisis. The Critical Access Hospital program, the Rural Emergency Hospital designation, the rural GME carve-outs: every one of these represents money flowing to institutions, and every attempt to reform them is met with the same argument — that any change will close hospitals and kill patients.
The result is a policy landscape where the problem is never defined with real metrics, the funding is never tied to measurable access outcomes, and the same institutions that absorb billions in rural subsidies also lobby aggressively against meaningful legislation like site-neutral payment reform. Health systems swallow enormous amounts of federal funding and still cannot completely close the remaining access gaps. (What they can do, and do very effectively, is drive up the cost of care for everyone else.)
There are many other levers to pull on if we want to be truly exceptional and improve rural access for the 11.7 million Americans who remain relatively underserved. I hope I’ve convinced you that the simple Canadian option offered up by many would take us backwards, not forward. There are some far more sensible options that should have wide public support.
First, it would seem a smarter and a better long term solution to solve the physician scarcity problem in rural areas by allowing for those who grow up in these communities to travel a vastly accelerated path to becoming a general practitioner. At the moment a bright young kid in rural West Virginia is much more likely to run his own HVAC shop than run his own primary care practice. Any current primary care practitioner will tell you the HVAC route is a much smarter and more lucrative path than a route to becoming a physician that has you spending a minimum of 11 years after graduating from high school and accruing mid six figures worth of debt. It wasn’t always that way — a century ago, a young person could go from high school to practicing medicine in five or six years, and many of those physicians served exactly these kinds of communities. So Megan and Razib’s comment on physician shortages and the need for high skilled immigrant labor that isn’t possible to be sourced locally has a lot of layers to it. The “shortage” is partly a function of funding a lot of residency spots in rural areas, that are then filled by overseas physicians looking for an entry point to the US health care system. This framework is a policy choice that doesn’t even do a good job of ever fixing the problem because physicians from Lahore and Hyderabad (or their children, who overwhelmingly leave medicine/ choose to practice medicine in metropolitan areas) only stay in these communities if they have no other option. If we, for instance, stopped funding rural residency slots, these hospitals that are still awash in cash from a variety of other federal programs would choose different labor options (nurse practitioners/physician assistants/pay more to local family practice doctors to help staff patients), and suddenly you would have a very different looking landscape of “need” for physicians. Bottom line: if you are going to try to engineer something — make it more attractive for local members of the community to become physicians in their community rather than massively incentivizing rural hospitals to import physicians to fill a need that you created.
Second, if we are to use American tax dollars to close the rural access gap, we need to demand better outcomes. The data exists to measure, county by county, how far Americans actually are from emergency cardiac care, primary care, and basic surgical services. Tie funding to some mix of those measurements. If a rural health system is receiving cost-based reimbursement, GME training slots, and Rural Emergency Hospital subsidies, it should be required to demonstrate what access it is providing — next-day primary care appointments, 24/7 emergency coverage, PCI capability — and lose its designation (and funding) if it cannot.
Third, since we actually need more hospitals, we should break the monopoly C-suite has on the opening of new hospitals. The physician hospital ownership ban — a product of the Affordable Care Act, lobbied for by the hospital industry — prevents the people most likely to solve rural access problems from doing so. Physicians from rural communities who want to raise capital, build facilities, and deliver care are legally prohibited from owning the hospitals they would staff. The ban protects incumbent health systems from competition. It does nothing for patients. Consider what happens where physicians can own facilities: Atlas Surgery Center in Amherst, New York — a physician-owned ambulatory surgery center built by the neurosurgeons of University at Buffalo Neurosurgery — performs same-day awake endovascular neurosurgery, carotid stenting, Gamma Knife radiosurgery, and complex spine procedures that would otherwise require multi-day hospital admissions at far greater cost. It is the first ambulatory center in the country to offer outpatient Gamma Knife. That is what physician ownership produces when the law allows it. Now imagine that model applied to rural communities that need a hospital and have physicians willing to build one. Currently, the law says no.
The entire rural access debate is premised on the assumption that only large health systems backed by federal subsidies can deliver care in underserved areas. The evidence for this is thin. What the evidence actually shows is that when physicians are allowed to own and operate facilities — ambulatory surgery centers, imaging centers, urgent care networks — they deliver care at lower cost with comparable or better outcomes. Extending that model to hospital ownership in underserved areas is the most direct path to closing the remaining access gaps without the perpetual subsidy machine that has manifestly failed to close them over three decades.
The mountain to climb is high. The first step may be the hardest: cutting through the noise of motivated academics who control most of the messaging on health policy and healthcare access. The public should have a clear understanding that the crisis narrative they have been sold is not a description of reality but a product — manufactured by those who profit from it, whether in funding or in political capital. Should we try to do it even better? Of course.
But there is little hope of getting anywhere without a good grasp of the scope of the problem that faces us.
Anish Koka is a Cardiologist in Philadelphia. He writes on medicine and health policy on his substack where this was originally published and also cohosts a weekly podcast : The Doctors Lounge
Link to PCI access US/Canada Interactive maps | More on map methodology, limitations